IVDD
Publication Date: 2015-04-12
History
8 year old Australian Sheperd, paraparesis for the last 3 days, is now non ambulatory with some motor function in his pelvic limbs
5 images
Findings
Orthogonal radiographs of the thoracolumbar spine are available for interpretation.
The previously noted mineralized intervertebral disc at the level of T12-T 13 and T 13-L1 remain visible but are in situ and do not appear to protrude into the spinal canal. There is mild ventral spondylosis at the level of L1-L2 and L2-L3. At the level of L4-L5 a faint area of mineralization is noted within the spinal canal just above the intervertebral disc. At this level, the intervertebral disc space is mildly narrowed. A urinary catheter is visualized. There is significant pulmonary atelectasis and resulting mediastinal shift of the cardiac silhouette appreciated on the ventral dorsal projection of the thorax.
Impression: 1. The changes described above at the level of L4-L5 are suggestive of presence of partially mineralized material within the lumen of the spinal canal. 2. Intervertebral disc mineralization as described above and associated ventral spondylosis. 3. Urinary catheter. 4. Pulmonary atelectasis secondary to general anesthesia.
For further evaluation if clinically indicated, advanced imaging such as MRI or CT could be useful.
MRI
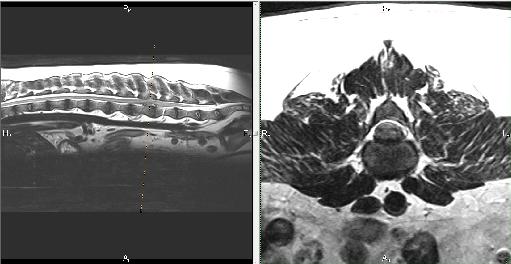
An MRI of the thoracolumbar spine was performed with the patient under general anesthesia. Images were obtained in multiple planes and sequences.
On the sagittal sequences, there is a large amount of well-defined, irregular material within the ventral spinal canal at the level of the mid-vertebral body of L4, extending to the intervertebral disc space of L4-L5. This material is of mixed signal, with portions being hypo to isointense to the spinal cord parenchyma on T2 sequences. This material is causing dorsal deviation of the spinal cord at this level, with complete loss of the ventral epidural signal. At this level, there is complete loss of the ventral and dorsal aspect of the spinal column on the HASTE sequence. The signal cranial to the lesion is decreased in intensity up until the thoracolumbar junction. On transverse sequences, this material within the ventral aspect of the spinal canal is causing severe compression of the spinal cord parenchyma. Along the cranial aspect of the material, the spinal cord is being compressed towards the left; however, in the central region of L4, the compression is from all along the ventral aspect. The disc material is causing >50% compression of the spinal cord parenchyma. Moving further caudal, the compression of the spinal cord is towards the right side.
The nerve roots are normal in appearance with no obvious compression. The intervertebral disc space at L4-L5 is decreased in comparison to the disc spaces surrounding it. Caudal to the lesion, there is mild, linear hyperintensity within the central region of the spinal cord parenchyma on the STIR sequence.
Impression: The described changes at the level of L4-L5 are consistent with intervertebral disc extrusion with severe compression of the spinal cord parenchyma.
Notes
Files